
Here’s the truth most pre-med advisors haven’t caught up to yet. If you’re applying to medical school in 2026, AI has already rewired your path. It reads your application before any human looks at it. It’s taught right now in 77 percent of US and Canadian med schools. And it sits next to cardiologists and pathologists in real exam rooms, doing work nobody trained those doctors to share with software a decade ago. Your competition? They’re using it too. Some smartly. Some in ways that get their files quietly killed before any reviewer opens them.
The real question isn’t whether AI affects your pre-med path. Obviously it does. What you actually have to figure out is how to position yourself for a healthcare system where AI sits in every layer. From the admissions software scanning your essay this fall, to the bedside decision tool your future attending will tap into on morning rounds, AI is already in the loop. Pretending it isn’t is a losing strategy.
The key takeaways from this guide:
• AI now screens more than 80 percent of US college applications before any human reads them
• 68 percent of colleges use AI essay detection tools to flag generated content
• 77 percent of US and Canadian medical schools already teach AI in their curriculum
• Authenticity, not polish, is what wins in the 2026 admissions cycle
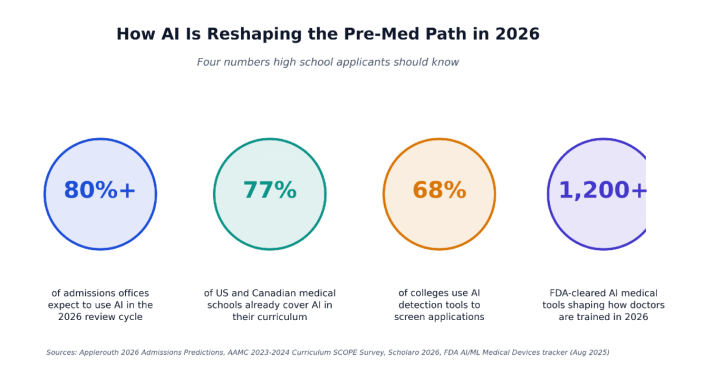
Four numbers shaping the 2026 pre-med admissions landscape
How AI Is Reshaping Medical School Admissions Today
From Human Reviewer To Algorithm-First Screening
Want a real example of how AI now reads applications? Look at Virginia Tech. The school pairs each file with one human reviewer and one AI system. A second human only gets pulled in when those two scores disagree by more than two points. More than 80 percent of US college admissions offices will run a similar setup in their 2026 cycle. Common App volume jumped 9 percent last year. Human reviewers couldn’t have kept up alone. AI isn’t replacing them. It’s doing the first read so the humans can spend their time on the borderline files that actually need a person.
Narrative coherence beats activity stacking
So what’s the AI actually scanning for? Coherence. One word. Whether your transcript, activities, essays, and rec letters all point at the same authentic healthcare story. An applicant with a clear thread beats an applicant with twice the activities and no story behind any of them, every time. The old game of activity stacking, that long shallow list of clubs and one-day volunteer gigs families used to chase, doesn’t help you anymore. It hurts you. Both AI and human readers spot the pattern in under five minutes.
Is AI Reading Your Personal Statement Before Any Human Does?
Yes. And it may be doing more than just reading.
How Essay Ai Detection Actually Works
Roughly 7 in 10 colleges now run AI detection as part of essay review. NACAC updated its ethics guide in fall 2025 to address this head-on. The software looks for stylometric patterns, sentence rhythms, vocabulary distribution. Things AI tends to do the same way every time. Here’s the part most applicants miss completely. Run your ChatGPT draft through three rounds of edits, swap some words, restructure a few paragraphs, and the underlying fingerprints still show up. Detection got better faster than rewrite habits did. That’s why so many of the essays flagged in 2024 came from students who genuinely thought they’d cleaned theirs up. They hadn’t.
What admissions officers want to see in 2026
US News covered 2026 med school trends and put it about as bluntly as anyone could. Authenticity beats polish. Period. Admissions officers want personal narratives that show actual reflection. The talk with a patient who said something that stuck with you for months. Your grandmother’s medication confusion that led to your first hospital visit at fourteen. That kind of specific lived detail can’t be generated. It has to be earned, lived through, and written in your own voice. After three or four hours reading a hundred AI-drafted essays in one sitting, every reviewer starts to feel like they’re reading the same essay with different names on it.
Why Medical Schools Already Expect You to Know AI
AI literacy is now an admissions signal
The AAMC’s most recent Curriculum SCOPE Survey laid it out: 77 percent of US and Canadian MD and DO programs already teach AI as part of their formal curriculum. The Miller School of Medicine hosted the IME 2026 Conference in March, and the whole conference focused on AI in med ed and clinical assessment. Notice the shift. Schools stopped asking whether they should teach AI. They moved on to asking how. Which means they want applicants who already get the lay of the land, not students whose first AI class will start in week one of their MS1 year.
What AI literacy looks like for a 17-year-old
AI literacy for a 17-year-old doesn’t mean coding. Nobody expects you to build neural networks. What schools actually want is for you to understand how AI shows up in actual hospitals right now. A radiologist sees a chest CT with thousands of slices and AI quietly flags the suspicious lung nodule before the radiologist gets to slide 47. An AI reads an ECG in three seconds, then a cardiologist adds the clinical context the algorithm has no way to know. A pathologist scans a biopsy slide algorithmically, then pulls up the result and makes the final call on a cancer diagnosis. If you can talk about that, acknowledge where AI still gets things wrong, and explain why human judgment isn’t going anywhere anytime soon, you signal exactly the kind of mind schools want to admit.
Want to go deeper than headline summaries? This ongoing review of healthcare blogs covers diagnostics, radiology, automation, and the boundaries clinicians still draw around the tech. Read even a handful of pieces from there and you’ll be miles ahead of peers who only memorised the talking points without context to back them up.
Will AI Replace the Doctor You Want to Become?
Short answer: no. But the role itself is shifting in ways every pre-med really should understand before they commit four years and roughly a hundred thousand dollars to the path.
Tasks versus roles: a critical distinction
The FDA has cleared over 1,200 AI medical algorithms so far. These tools sit alongside doctors in radiology, in pathology, in cardiology clinics, and increasingly in chronic disease management apps too. But none of them sign off on the final diagnosis. That’s still the physician’s call. And it probably will be for the next decade at least. AI is replacing tasks, not roles. The cardiologist practising in 2030 will use AI tools every workday and still be the doctor making the call.
What AI looks like across the specialties you might choose
Modern cardiology practice runs AI for ECG interpretation, echocardiogram analysis, and risk modelling. But the cardiologist still explains the result to the patient face to face, negotiates a treatment plan with the family, and decides what to do when the AI model and the clinical picture flatly disagree. That last bit happens way more often than the AI vendors like to admit.
Mental health gives us another clean example. Take Wysa and Woebot. Both are AI-powered cognitive behavioural therapy apps. Both earned FDA Breakthrough Device status. They deliver structured therapy through text conversations and often bridge the six-to-eight-week wait patients face before they can see a licensed human therapist. Replace psychiatrists? No, nowhere close. But they expand access for people who would otherwise get nothing, especially in underserved areas where the wait stretches past three months.
The business side of practice is shifting too. AI now sits inside healthcare billing, coding, and revenue cycle workflows across multiple medical specialties, stripping hours of admin work out of a physician’s week and pushing the actual practice of medicine back toward patient care. Which is presumably why most of you signed up for this path in the first place. Not the billing software.
How to Use AI Ethically as a Pre-Med Applicant
Where AI genuinely helps
Used the right way, AI is a genuinely powerful study partner. It will explain an MCAT-level concept on demand. Generate practice questions targeted at your specific weak spots. Walk you through a chemistry or biology problem set at the exact pace your brain needs. Help you map study plans week by week, then adjust them when you fall behind. For students who can’t afford a $4,000 private tutor, AI delivers real access to high-quality study support. Up until two years ago, this kind of help simply didn’t exist at this price. UWorld AI, Blueprint, ApexVision, the personalised MCAT prep market is now mainstream.
Where AI quietly hurts your application
Using AI to draft your personal statement or scholarship essay is application fraud at most US universities. Period. The same goes for inventing activities you never actually did, generating patient interactions that never happened, or having AI write rec letters that should come from a teacher who knows your face. Even when these tactics slip past the first round of detection, they almost always produce content so generic it disappears in the pile. Reviewers can usually tell within two paragraphs. Within two paragraphs. The table below breaks down where AI helps and where it quietly torches your application.
| AI Use Case | Responsible Practice | Pitfall to Avoid |
| Personal statement | Brainstorming, outlining | Generating the full draft |
| MCAT / SAT prep | Practice questions, weak-spot review | Cheating on real practice exams |
| Activity descriptions | Editing for clarity | Inventing fake activities |
| Interview prep | Mock practice on common questions | Memorizing scripted answers |
| Research and essays | Citation help, structure feedback | Generating original analysis |
What Pre-Med Applicants Should Do in 2026
- Build real AI literacy. Know how AI works in medicine today, what it does well, where it stumbles, and where doctors still don’t trust it. Don’t fake fluency. Interviewers will catch you in 30 seconds.
- Document authentic clinical exposure. Quality of reflection beats hours of shadowing every single time. Even at top programmes.
- Write in your own voice. Draft essays yourself. Revise them yourself. Share only with mentors who know you well enough to call you out when something rings false.
- Take on a structured AI-in-medicine project. Online courses, local lab research, independent reading, any of those count. The key is being able to talk about what you actually learned and how it changed how you think.
- Lean into what AI can’t do. Empathy. Ethical judgment under pressure. Complex patient communication when the stakes are high. These are your strongest applicant signals in 2026, and they’ll likely stay that way through 2035.
Author Bio
Isaac is a highly accomplished healthcare professional with over 13 years of experience in healthcare administration, clinical operations, and patient education. He holds a bachelor’s degree in Health Administration and has built his career around making healthcare more accessible and understandable for everyday patients. Earlier in his career, he worked at a large multi-physician family care and occupational health practice with two locations in northwestern Pennsylvania, where he developed deep expertise in patient flow, clinical documentation, and primary care operations.
Today, Isaac contributes to Marham.pk’s editorial team, writing and reviewing patient education articles across Marham’s core specialties, including General Physician, Gynecology & Obstetrics, Dermatology, Pediatrics, Cardiology, Gastroenterology, Endocrinology, Psychiatry, ENT, Orthopedic Surgery, Urology, and Internal Medicine. His focus is making complex medical information accessible to Pakistani patients so they can confidently choose the right doctor, book the right lab test, and ask the right questions in a consultation.
